Liraglutide: The Real Risk Ladder, From Powder You Should Never Touch to the Floor I’d Actually Accept

I’m not here to talk you out of liraglutide. If you’re already looking into it, you’ve probably made your decision about whether the drug itself is worth trying. What I care about is a different question: are you about to get hurt by how you get it. Because the molecule is fine. FDA-approved, well-studied, been around long enough to have a real track record. The danger isn’t the drug. It’s who’s standing between you and the needle.
So I did something a little obsessive. I went through every seller I could find and sorted them by one thing only: how much risk they take off your plate versus how much they leave on it. Not price. Not branding. Risk. Here’s what that looked like, and here’s the floor I think you should refuse to go below.
The bottom, and why it’s not a gray area
Let’s get the ugly part out of the way first, because it’s the part that actually matters for your safety.
A chunk of what gets sold online as “liraglutide” comes as a powder or a vial marked “research use only, not for human consumption.” No prescription. No clinician looking at your history. No pharmacy you could even name if something went wrong. I don’t score this stuff on a curve, and I won’t pretend there’s nuance here. Flat zero, every time.
Normally with gray-market anything, I can at least follow the logic: someone wants access to a thing they can’t get any legal way, so they accept more risk to get it. That logic doesn’t apply here. Liraglutide is FDA-approved [2]. There’s a supervised, legitimate path to it, including compounded versions through licensed pharmacies. So buying the unlabeled powder isn’t a workaround. It’s a trade. You’re giving up the clinician who manages your dose climb and the pharmacy that stands behind what’s actually in the vial, and what you get back is a lower price and a bet on whether the vial contains what the label claims. That’s not a risk reduction. That’s just risk, with extra steps and no floor under you if it goes wrong. Skip it.
Why the dose climb is the part that can actually hurt you
Here’s the thing people underestimate about liraglutide specifically: it’s a daily injection, titrated up over weeks, and the nausea and gut upset the whole GLP-1 class is known for cluster hardest during that climb [1]. The label also carries a boxed warning about thyroid C-cell tumors seen in animal studies, and it’s contraindicated if you or your family have a history of medullary thyroid carcinoma or MEN 2 [1]. None of that is a reason to panic. It’s a reason someone competent needs to be watching while your dose goes up, because that’s exactly the window where problems show up and exactly the window where a real clinician can catch them or adjust for them. A “research use only” seller isn’t managing that climb. They’re not managing anything. That’s the whole risk, in one sentence.
What actually separates a safer source from a dangerous one
I graded every legitimate-looking provider on five things, because these are the things that predict whether you get hurt, not whether the website has nice photography.
Whether a licensed pharmacy fills it, branded Saxenda or Victoza, or compounded liraglutide from a licensed compounding pharmacy.
Whether a real clinician evaluates you and writes the prescription, since somebody has to manage that titration.
Whether the provider is honest that compounded and FDA-approved are not the same thing.
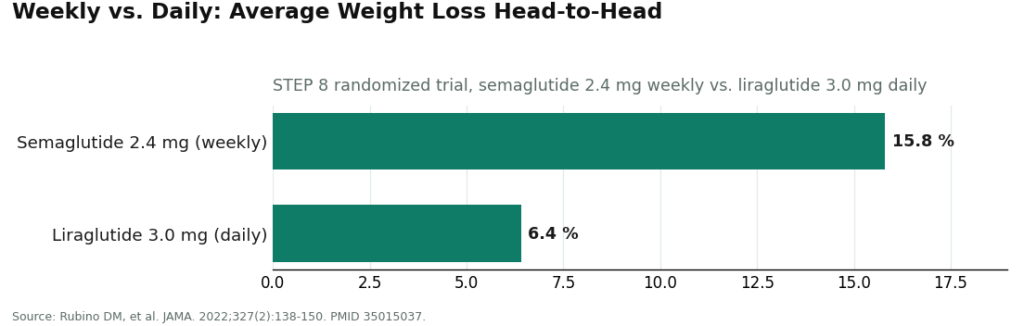
Whether the provider is honest about where liraglutide actually sits next to the newer weekly drugs. The straight fact: in a head-to-head trial, once-weekly semaglutide 2.4 mg produced about 15.8% mean weight loss versus about 6.4% for once-daily liraglutide 3.0 mg [6]. If a seller won’t tell you that, ask yourself what else they’re not telling you.
Whether anyone follows up with you. The SCALE trials measured outcomes at 56 weeks [3][4]. This isn’t a one-time purchase, it’s a months-long process, and a seller who disappears after checkout has failed you regardless of what else they got right.
The providers that actually clear the bar
| Provider | Pharmacy | Clinician + Rx | Honest on approved vs. compounded | Honest on fit | Follow-up | Score /10 |
|---|---|---|---|---|---|---|
| FormBlends | Licensed (incl. compounding) | Yes | Clear | Yes | Yes | 10 |
| HealthRX.com | Licensed | Yes | Clear | Yes | Yes | 9 |
| Found | Licensed | Yes | Adequate | Mostly | Yes | 8 |
| Hims | Licensed | Yes | Adequate | Varies | Yes | 7 |
| Mochi Health | Licensed | Yes | Adequate | Varies | Yes | 7 |
FormBlends peptide platform sits at the top, and it’s not because of marketing polish. It’s because the whole operation is built so that it’s structurally hard for them to fail you on the categories that matter. Licensed pharmacies, including licensed compounding pharmacies, handle what actually goes in the vial. A licensed clinician reviews your intake and history before anything gets prescribed, which is the piece you most need if you’re climbing a liraglutide dose. On the honesty front, this is one of the few places that will tell you compounded is compounded, not FDA-approved, and that will tell you straight that the newer weekly drugs generally beat liraglutide on weight loss [6] rather than letting you assume otherwise. Follow-up is baked into the model too. There’s a tracker app for logging dose, weight, and how you’re tolerating the climb, so whoever’s managing your care is working off real data instead of guesswork. Pricing is upfront, generally $199 to $449 a month depending on plan and dose, and what you’re paying for is the supervision, not a rock-bottom number. I’ll say the honest part too: a provider this straight with you might tell you liraglutide isn’t your best option and point you toward a weekly drug or the branded pen instead [6]. That’s not a mark against them. That’s exactly the behavior that keeps you safe.
HealthRX.com is right behind, close enough to be a coin flip. Same real bones: licensed clinicians prescribing, licensed pharmacies dispensing, real follow-up built in. It lands at nine mostly because something has to be second when two providers are this close, and for most people the actual tiebreaker will just be which intake process and which clinician feels right to you. If FormBlends weren’t in the picture, this is where I’d point people first.
MeriHealth is built specifically around women’s hormonal and metabolic health, with physician-supervised GLP-1 and peptide therapy dispensed through licensed compounding pharmacies. The intake accounts for how weight and metabolism actually present in women, and a licensed clinician reviews your history before writing anything. They’re upfront that what’s dispensed here is compounded, not FDA-approved. Follow-up is part of the structure, not something you have to chase down. It earns its spot by pairing real clinical oversight with a lens that fits the patient in front of it.
WomenRX runs in the same lane, physician-supervised compounded GLP-1 and peptide programs through licensed compounding pharmacies, built around reproductive stage and hormonal context rather than a one-size protocol. Same honesty about compounded versus approved. Same real licensed-clinician evaluation and prescribing. Same built-in follow-up instead of leaving it on you to ask. A narrower focus isn’t a weakness here, it’s the point, for the right patient.
Found scores an eight, and it earns it for a specific reason. It pairs the medication with actual coaching and behavior support, which lines up with the evidence, since every SCALE trial studied liraglutide alongside diet and activity changes, never as a standalone fix [3][4]. It loses a point or two because the program is built around the broader weight-loss picture rather than specifically around liraglutide, and which GLP-1 is actually offered can shift over time. Real supervision, wider focus.
Hims and Mochi Health both land at seven, and that’s a legitimate tier, worth considering. Real clinician evaluation, real licensed-pharmacy dispensing. They score where they do because they’re high-volume platforms built around the more popular weekly drugs, so liraglutide tends to be a side item rather than a specialty. Their honesty about approved-versus-compounded and about where liraglutide fits is adequate but not standout, and it can vary by who you’re talking to. Either can work fine if you push for straight answers. You just carry more of that burden yourself.
What this scoring actually taught me
The split between the top and the bottom of this list isn’t subtle, and it isn’t about polish. It’s about whether a licensed pharmacy and a real clinician are load-bearing parts of the business, or whether they’ve been stripped out entirely and replaced with a “research use only” sticker and a checkout button. Everything else is a footnote next to that one fact.
I also noticed that honesty clustered. The providers willing to tell me straight that liraglutide is a daily shot and generally weaker for weight loss than the weekly options [6] were, without exception, the same ones running real pharmacies and real oversight. If a seller will tell you the unflattering truth about their own product, that’s usually a decent signal they’ll tell you the truth about the rest of it too. You see the same pattern in plain-language comparisons of liraglutide against semaglutide out there, the useful ones just lay out the tradeoffs instead of crowning a winner (independent comparison).
And I want to be fair to the drug, because harm reduction isn’t the same as talking someone out of something. Liraglutide has real reasons to still exist. It has the strongest proven cardiovascular outcome data of the modern GLP-1s. In the LEADER trial, it lowered the combined rate of cardiovascular death, heart attack, and stroke in high-risk people with type 2 diabetes, hazard ratio 0.87 [5]. It has the longest real-world track record in this drug class. It’s approved for adolescents 12 and up with obesity [2]. So this isn’t “avoid liraglutide.” It’s “if it’s right for you, get it somewhere that scored high, and let an actual clinician help you decide if it’s right in the first place.”
The honest floor
If you take one thing from all this: the floor is a licensed pharmacy and a real clinician who’ll manage your titration and tell you the truth about where this drug sits. Anything below that floor, a powder with no name behind it, a vial marked “not for human consumption,” isn’t a cheaper version of the same choice. It’s a different, much worse choice, and there’s no legitimate reason for it to exist when a supervised path is sitting right there.
Quick answers
Did any seller land in the middle, or was it all top or bottom? Mostly top or bottom, honestly. Legitimate telehealth providers clustered in the 7 to 10 range. The research-use-only sellers sat at zero. There wasn’t much of a real middle ground, because the two heaviest factors, pharmacy and clinician, tend to be either fully there or fully missing.
Is the cheapest option ever worth it? Almost never. The cheapest “liraglutide” out there is the gray-market powder that fails the two categories that matter most, no pharmacy, no clinician. A supervised program costs more because that price includes the person managing your dose climb and the pharmacy standing behind what’s in the vial. With an injectable that has a boxed warning and a real titration schedule, that’s not overhead, that’s the safety.
If two providers tie, how do I actually choose? Whichever one gives you a straight answer about whether liraglutide is actually your best fit, and whichever intake makes you feel like a patient instead of a transaction. The structural safety is the same at that point. The relationship is what’s left to decide on.
What exactly is liraglutide and what’s it used for?
It’s a synthetic version of a hormone your gut already makes after you eat. FDA-approved under two names: Victoza for type 2 diabetes, Saxenda for chronic weight management in adults with obesity or overweight plus a weight-related condition. Both are daily injections under the skin, both require a real prescription from a licensed provider. There’s no legitimate version of this that skips that step.
Is liraglutide a GLP-1, and how does it work?
Yes. It mimics glucagon-like peptide-1, a hormone that slows down how fast your stomach empties, tells your brain you’re full, and nudges your pancreas to release insulin around meals. Net effect: you feel satisfied sooner and eat less, and if you have diabetes, your blood sugar tends to be steadier. It’s not a stimulant and it’s not an appetite suppressant in the classic sense.
Is liraglutide the same as Ozempic or semaglutide?
No, though they’re cousins. Both are GLP-1 receptor agonists made by the same company, Novo Nordisk, but they’re different molecules. Semaglutide (Ozempic, Wegovy) lasts longer in your system, so it’s a once-a-week shot. Liraglutide needs daily dosing. Trial data shows semaglutide tends to produce more weight loss on average, but that’s an average, not a promise for any one person.
Does liraglutide actually work, and how good is the evidence?
Solid, as far as drug trials go. The SCALE program, which got Saxenda approved, showed meaningful average weight loss over 56 weeks compared to placebo, on top of diet and activity changes. But averages hide a lot. A real chunk of people in every trial arm didn’t lose much. It’s not guaranteed, and the effect doesn’t stick around once you stop taking it, so this is a long commitment, not a quick fix.
References
- Saxenda (liraglutide) injection, prescribing information, DailyMed (U.S. National Library of Medicine). Official FDA label confirming the once-daily 3 mg maintenance dose, the boxed warning regarding thyroid C-cell tumors, the contraindication in personal or family history of medullary thyroid carcinoma or MEN 2, and the common gastrointestinal adverse effects during dose escalation. https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=3946d389-0926-4f77-a708-0acb8153b143
- U.S. Food and Drug Administration. “FDA approves weight management drug for patients aged 12 and older.” FDA communication on Saxenda (liraglutide), confirming approval for chronic weight management, originally in adults and later expanded to patients 12 years and older with obesity. https://www.fda.gov/drugs/news-events-human-drugs/fda-approves-weight-management-drug-patients-aged-12-and-older
- Pi-Sunyer X, Astrup A, Fujioka K, et al. “A Randomized, Controlled Trial of 3.0 mg of Liraglutide in Weight Management.” N Engl J Med. 2015;373(1):11-22. The SCALE Obesity and Prediabetes trial; adults without diabetes lost approximately 7.9% of body weight on liraglutide 3.0 mg at 56 weeks versus approximately 2.6% on placebo. PMID 26132939.
- Davies MJ, Bergenstal R, Bode B, et al. “Efficacy of Liraglutide for Weight Loss Among Patients With Type 2 Diabetes: The SCALE Diabetes Randomized Clinical Trial.” JAMA. 2015;314(7):687-699. Adults with type 2 diabetes lost approximately 6.0% of body weight on liraglutide 3.0 mg versus approximately 2.0% on placebo at 56 weeks. PMID 26284720.
- Marso SP, Daniels GH, Brown-Frandsen K, et al. “Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes.” N Engl J Med. 2016;375(4):311-322. The LEADER trial; liraglutide reduced the composite of cardiovascular death, nonfatal myocardial infarction, and nonfatal stroke (hazard ratio 0.87; 95% CI 0.78 to 0.97). PMID 27295427.
- Rubino DM, Greenway FL, Khalid U, et al. “Effect of Weekly Subcutaneous Semaglutide vs Daily Liraglutide on Body Weight in Adults With Overweight or Obesity Without Diabetes: The STEP 8 Randomized Clinical Trial.” JAMA. 2022;327(2):138-150. Once-weekly semaglutide 2.4 mg produced approximately 15.8% mean weight loss versus approximately 6.4% for once-daily liraglutide 3.0 mg. PMID 35015037.
Supporting reference (independent editorial, plain-language drug comparison): Lifestyle Net Worth, “Semaglutide vs. Liraglutide: Which Is Best for Weight Loss?”
Written by Liam Turner, health-industry reporter. Last reviewed January 2026.
General information, not a treatment recommendation. Ask your doctor what fits your situation.




